The aim of this treatment is to remove the blockage in a narrowed artery in order to permit better blood circulation.
Procedure:
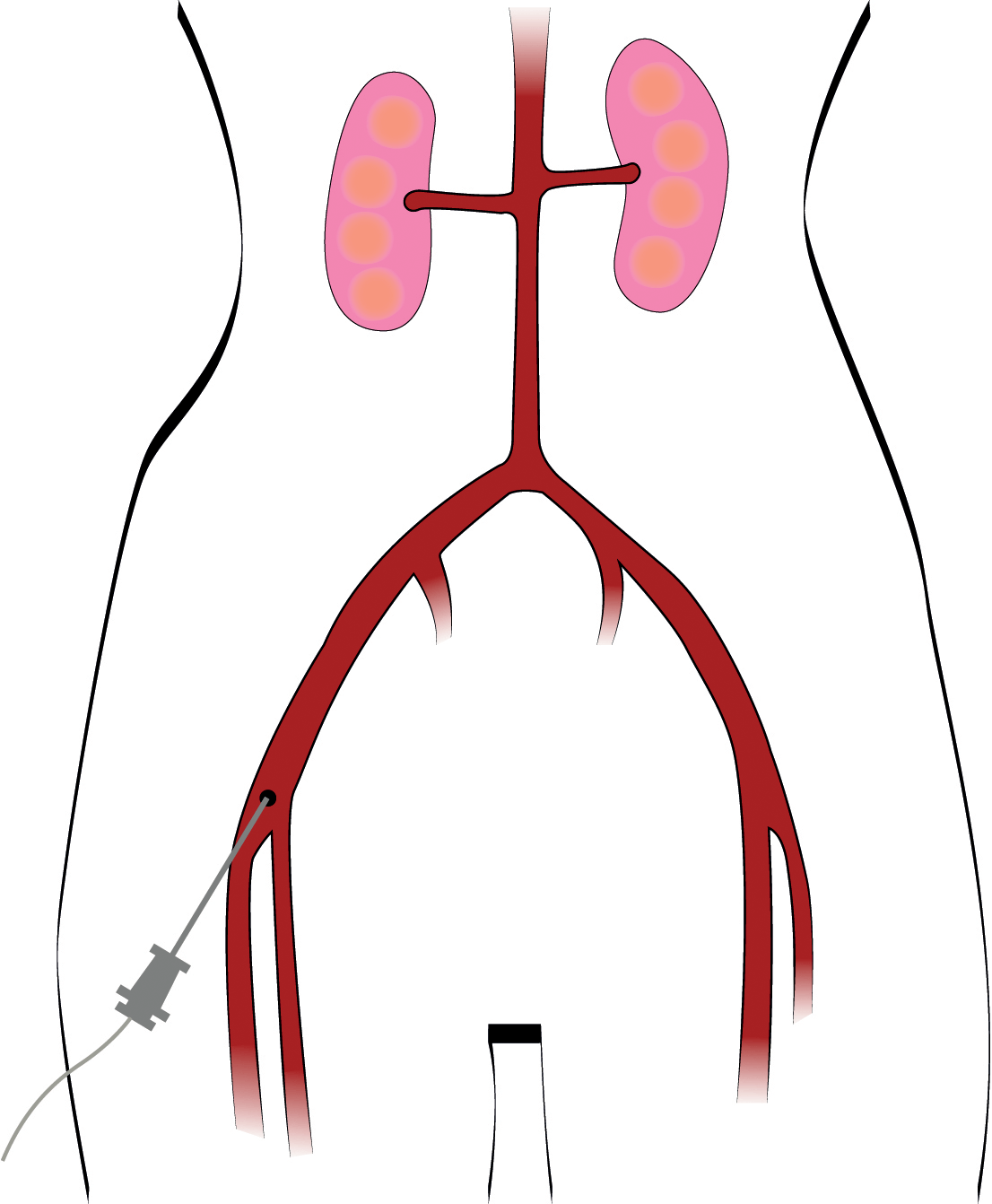
A catheter is inserted into the artery in the groin (but sometimes also in the arm).
By injecting a dye, the physician can follow the path of the catheter in the arteries with the help of X-rays (this is called fluoroscopy). The catheter is guided to the point where there is a narrowing of the artery. A tiny balloon is then advanced to the narrowed or blocked artery and gently inflated until the artery is sufficiently widened.
Other possibilities during treatment:
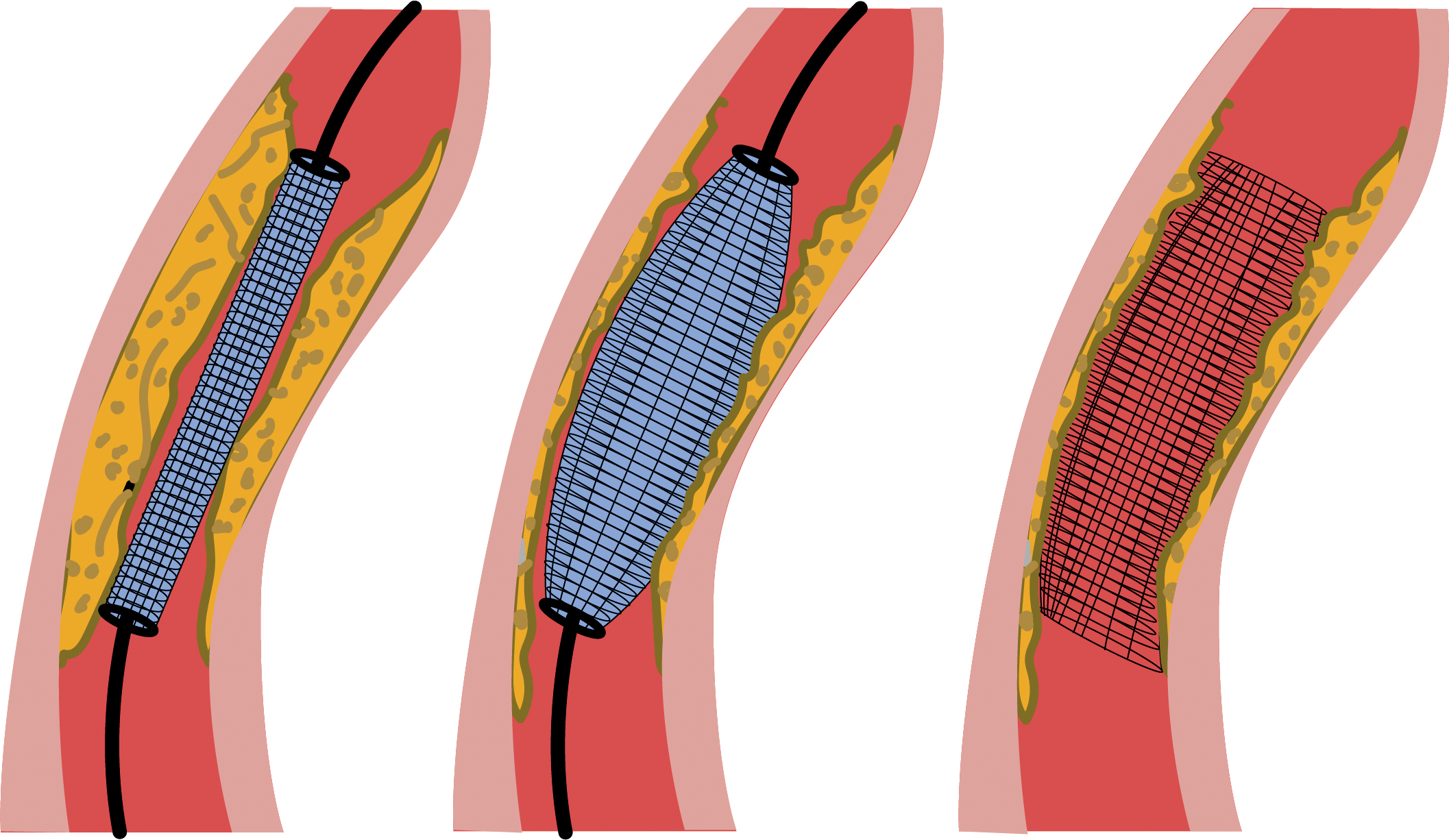
The physician may also insert a wire mesh tube called a “stent” inside the artery to decrease the chance of the artery narrowing again.
Percutaneous angioplasty is performed at the hospital and takes one to two hours. An overnight hospital stay is not necessary.
Potential complications:
Complications may occur, but they are rare. The healthcare team will monitor you for bleeding at the site where the catheter was inserted or for an allergic reaction to the dye. You can discuss this with your doctor.
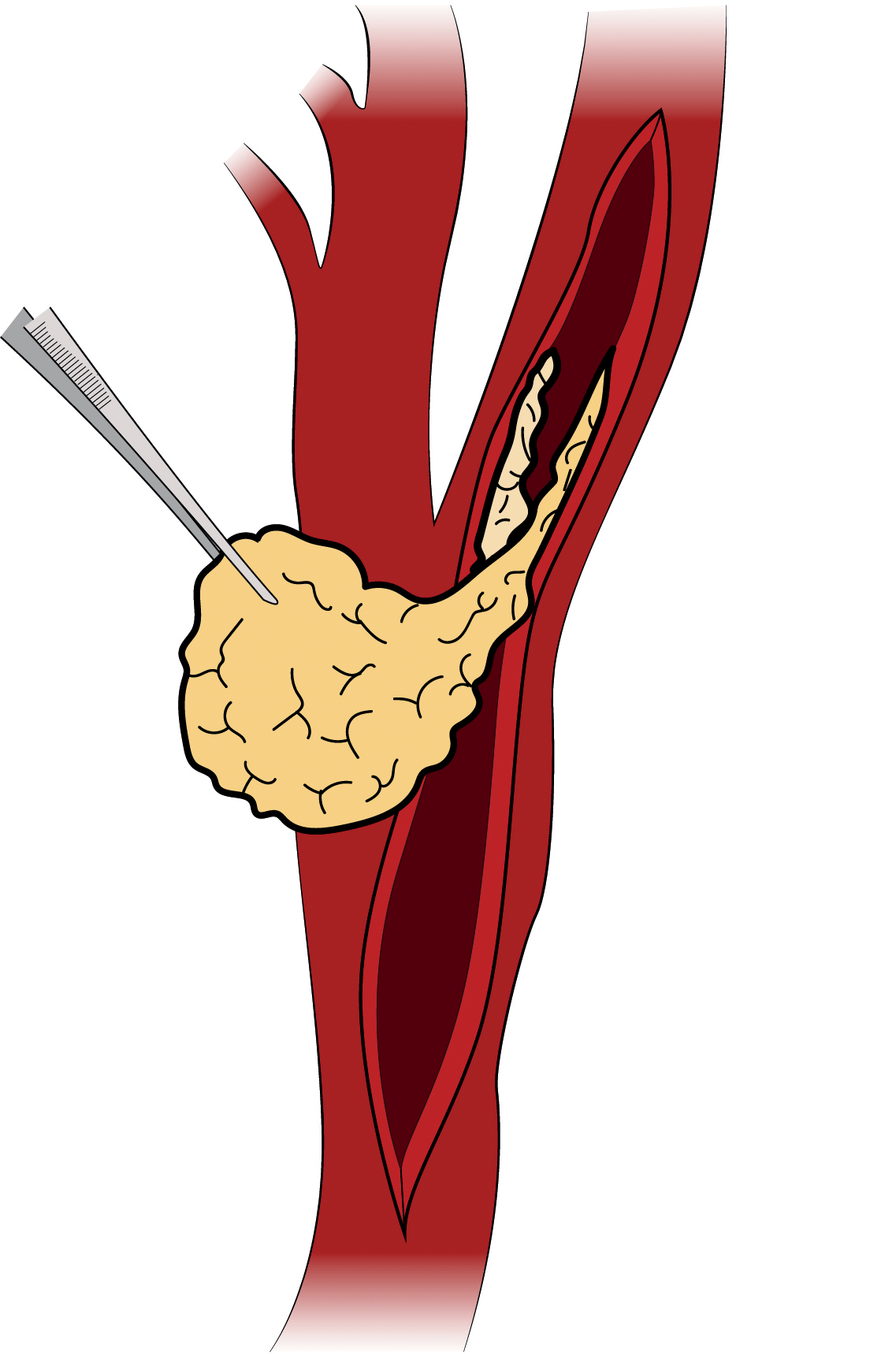
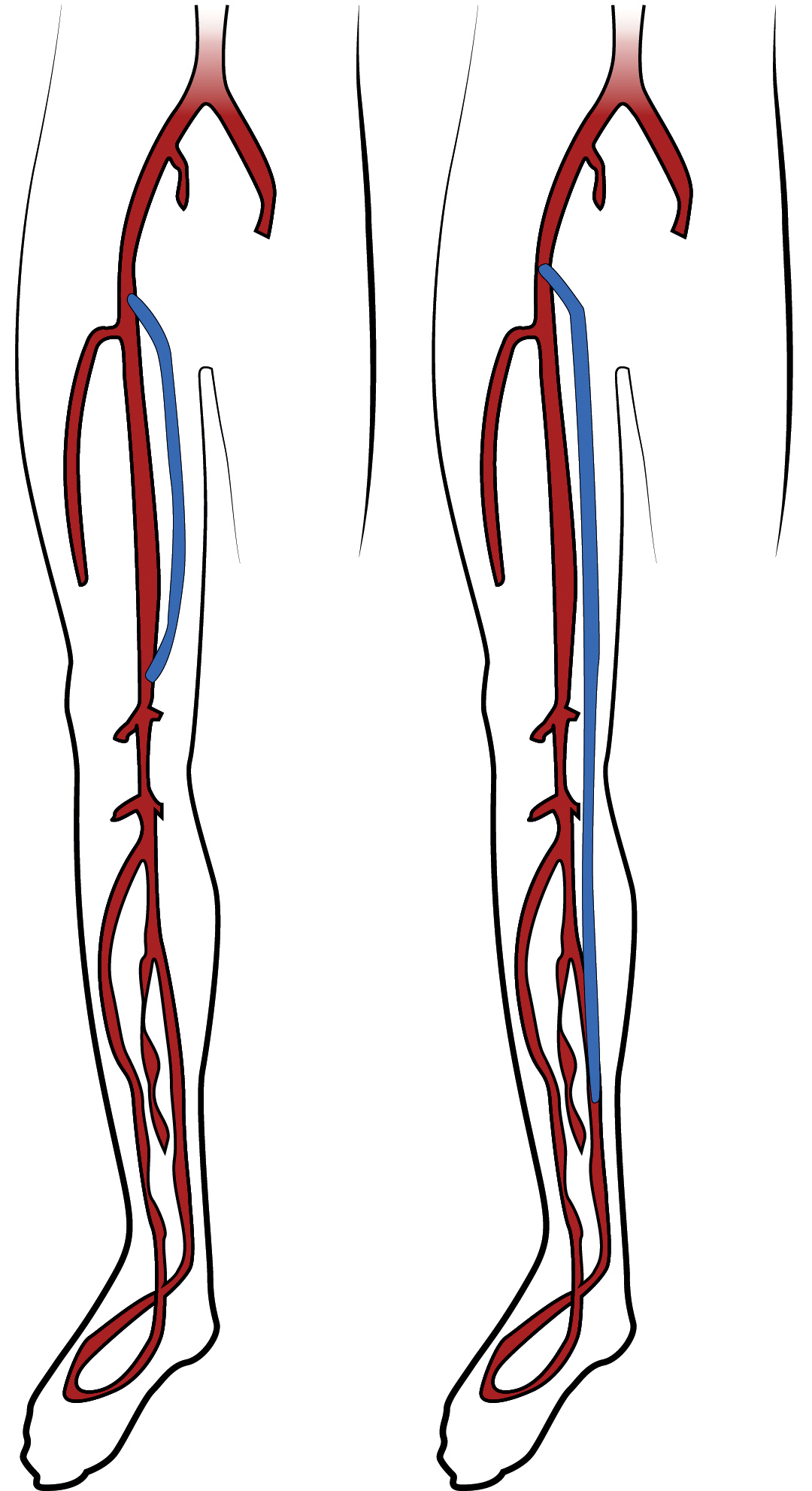
Surgical treatment is mainly aimed at restoring blood flow. Surgery is performed in an operating room.
Several tests and appointments are necessary prior to surgery (see the sections on physical examination and tests).